 ID: hksportsinstitute
ID: hksportsinstitute

Sports Medicine Education No. X - Meniscal Injury
Anatomy
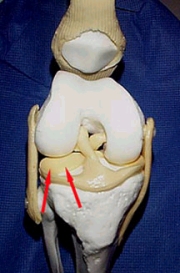
Fig 1: Lateral Meniscus (red arrow)
In the knee joint, you will find two C-shaped cartilage situated in between the lower end of the thighbone (femoral condyle) and upper end of the shinbone (tibial plateau).
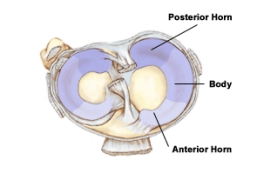
Fig 2: Superior View of the Menisci
Both menisci are C-shaped fibrocartilages triangular in cross section with the peripheral part being thickness and thinning towards the center. They function primarily as load distributors when we walk or run. The menisci also contribute to the knee's stability.
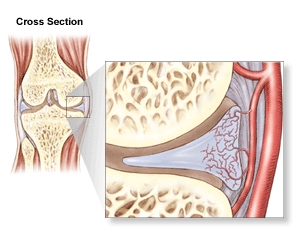
Fig 3: Blood Supply to the Meniscus
Only the peripheral part of the meniscus is supplied by nerve and blood vessel. Hence, pain may not be present in those with meniscal injury. Also, it hasminimal ability to heal by itself when injured.
Injury Mechanism
The meniscus is injured when a strong and sudden twisting force is applied to a bent knee in a weight bearing position. A classical example is, a basketball player jumps to catch the ball and lands with the knee inwardly rotated. Then he makes a fast turn towards the landing leg and results in a mensical injury. Meniscal injury may also be resulted from vigorous deep squatting, for example, repeated frog jumps.
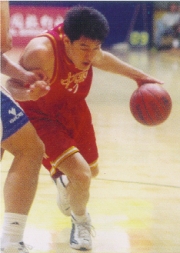
Fig. 4: Basketball players can injure their menisci when a strong and sudden twisting force is applied to a bent knee in a weight bearing position.
Signs and Symptoms
Signs and symptoms vary with the severity of injury. In general, one may feel or hear a 'pop' at the moment of injury, which may also be accompanied, with some degree of pain. Several hours later, swelling develops which will persist for sometime.
'Locking' of the knee is a common complaint. One may have difficulty in straightening the knee or bending the knee fully. These are caused by the entrapment of torn meniscal fragment inside the knee joint. The knee can suddenly lock on twisting and then unlock with an audible click.
On clinical examination, tenderness is felt over the joint line. With compression and twisting of the knee joint (McMurray's test), pain can be reproduced.Clicking might also be felt or heard. Another typical symptom is increased pain and swelling of the knee after it has been overloaded.

Fig 5: McMurray Test
Meniscal injury can also be objectively diagnosed with Magnetic Resonance Imaging (MRI) and Arthroscopy
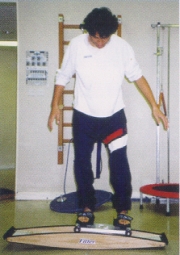
Fig 6: Arthroscopic View of Meniscal Tear
Types of Meniscal Injury
There are many classifications in meniscal injury. Simply speaking, it can be classified according to the location and pattern of tear. Common patterns of tear include bucket handle tear, radial tear, flap tear and complex tear. The type of tear and its severity directly govern the choice of treatment particularly when surgical repair is involved.
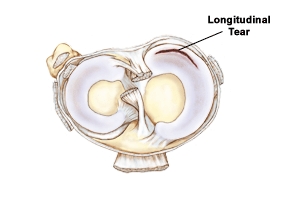
Fig 7: Meniscal Injury - Bucket-handle Tear
Management
All significant knee injuries should be evaluated by an Orthopedic Surgeon or Sports Physiotherapist. Features of significant knee injuries include severe pain or pop sound on injury, development of knee swelling, loss of knee range of motion, locking and give-way. The principle of 'R.I.C.E.' to control swelling is essential for the management of meniscal injury particularly in the first 24-48 hours. Although swelling is normal in a healing process but excessive swelling will impede the healing process. Hence controlling of swelling is essential.
For minor tear involving small portion at outer part of meniscus, self-healing may be possible. Rest to minimize the stress of the injured meniscus is extremely important. Light loading exercises for toning up muscles are permitted. When weight bearing is allowed, proprioceptive exercises, strength and conditioning exercises will be added progressively under supervision. Electrotherapy may also help to enhance the healing.
Surgery is indicated for symptoms of recurrent locking, swelling and pain. However, surgeon will try to save the meniscus as much as possible in order to preserve its weight bearing function. This can be achieved by partial menisectomy (to remove the torn fragment and preserve the completeness of meniscus) or by suturing the torn fragments back together.
Progressive exercises which restore the proprioception, strength and functional ability of the knee joint are the ultimate goals of the post-surgical rehabilitation.

Fig 8. Full recovery and return to pre-injury sporting activities are possible in 3-6 weeks for those with partial menisectomy and 8-12 weeks for those with meniscal repair.
The content of this leaflet is provided by:
Sports Medicine Department, Athlete & Scientific Services Division, Hong Kong Sports Institute
For more information, please contact:
Sports Medicine Department
Telephone: (852) 2681 6134
All information in this pamphlet is for reference only