 ID: hksportsinstitute
ID: hksportsinstitute

Sports Medicine Education No. IX - Neck Pain
Sports injuries involving cervical spine vary considerably in severity and nature from minor sprains and strains to catastrophic trauma resulting in either permanent or transient functional and neurological deficit. The information provided in this pamphlet focuses mainly on non-catastrophic cases.
Anatomy
Cervical spine (Fig.1) consists of seven vertebrae that are separated by intervertebral discs and are supported by ligaments and muscles. The cervical vertebrae articulate with each other and move according to the muscle contraction. The neck is a very mobile unit that also needs to support the heavy weight of the head. Hence it is susceptible to injury particular those resulting from excessive stress and strain.
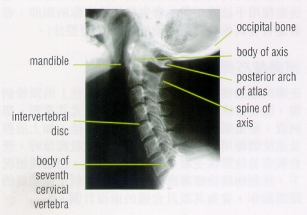
Figure 1: Lateral radiograph of cervical region of vertebral column
Mechanism of injuries
The most common types of traumatic injuries like sprains or strains are resulted from sudden acceleration, deceleration, or mild contact with an object such as the ground, an opponent, or the ball. Non-traumatic injuries (often classified as overuse injury) include poor posture or sustained postures; incorrect technique particularly in throwing or racquet sports, or poorly designed strengthening program which leads to muscle imbalance in the upper quarter of body.
Mechanisms of traumatic injury include:
-
Sudden hyperflexion may cause a compression fracture at the anterior cervical vertebrae and ligament injuries at the posterior side of the cervical spine.
-
Hyperextension injuries may occur in contact sports, falls and deceleration of dynamic flexion movements. Damage of anterior discs and ligaments and compressive fracture of the posterior vertebral bodies may be resulted.
-
Axial Compression injuries can happen in American football, diving and ice hockey. Subluxation, facet dislocation or fracture dislocation may result from the failure in discs, ligaments and bones.
-
High velocity accident can occur in car racing, skiing, speed skating and snowboarding. Collision will cause serious cervical injury and sometimes even death. Whiplash type injuries may also occur.
-
Forced excessive range of motion may occur during judo and wrestling when an athlete is forced into an awkward position by an opponent. Fracture/dislocation is unlikely in these situations but muscles, ligaments and nerves may be compromised.
-
Brachial plexus ( an area where the nerve from the spinal cord splits into individual arm nerves) injury may occur when compression or traction force is exerted on the cervical spine. It is not common in sports except American football and mountaineering when the nerves are injured by compression ( heavy backpacks) or traction ( collision with opponents ).
Signs and symptoms
Signs and symptoms, depending on area and severity of injury, may include pain, stiffness, weakness, pins & needles, nausea, dizziness, instability or loss of function. Other than localised pain, upper cervical spine problems may refer pain to the head whereas mid and lower cervical spine problems may refer symptoms to the upper limb.
Predisposing factors of non-traumatic neck pain in athletes
Poor upper quarter posture
Forward head posture (Fig.2) is the most common incorrect posture that contributes to cervical problems. This posture puts uneven stresses and overload on certain parts of the cervical spine where in turn are prone to dysfunction and develop cervical pain. A correct posture involves: chest lifted, shoulders relaxed, chin tucked in and head levelled. The neck should feel strong, straight and relaxed. Cervical pain or dysfunction may be further triggered or aggravated by sporting activities.

Figure 2a. Forward head posture

Figure 2b. correct posture
Muscle imbalance
Muscle imbalance and poor posture of the upper quarter have a strong relationship. One can be the result or the cause of the other. Muscle imbalance also affects movement co-ordination and may induce faulty stresses on the cervical spine. Upper trapezius, the pectorals and levator scapulae are commonly tight while the deep neck flexors and lower scapular muscles are commonly weak in athletes with cervical problems.
Treatment Protocol
Rest
An initial period of immobilisation with the use of cervical collar is indicated if the condition is irritable.
Medication
Non-steroidal anti-inflammatories, analgesics and muscle relaxants prescribed by the doctor are frequently helpful at the acute stage.
Physiotherapy
Physiotherapists may use mobilisation, manipulation, soft tissue mobilisation, electrotherapy and acupuncture to alleviate pain, restore mobility and relieve muscle spasm. Stretching of tight muscles (e.g. upper trapezius, the pectoral and the levator scapulae) (Fig.3) and strengthening of weak muscles (deep neck flexors and lower trapezius) might also be needed. Postural exercise might be done with correction and advice given as indicated.

Figure 3a: upper trapezius stretching exercise
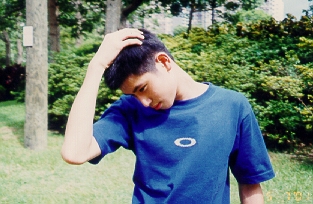
Figure 3b: levator scapulae stretching exercise
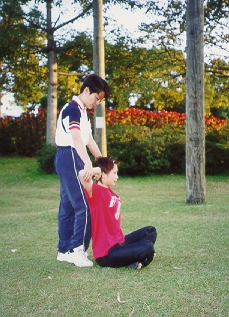
Figure 3c: pectoralis major & anterior deltoid stretching exercise
Manipulation
The use of manipulation of the spine to treat patients with pain involves a high velocity thrust. Manipulation of the spine differs from mobilisation of the spine because during manipulation of the spine, the rate of vertebral joint displacement does not allow the patient to prevent joint movement. Mobilisation of the cervical spine involves low velocity (non-thrust) passive motion that can be stopped by the patient. Because of the proximity of the vertebral artery to the lateral cervical articulations, caution must be taken during manipulation of the cervical spine. It is thought that stroke can be induced as a result of manipulation of the cervical spine by mechanical compression or excessive stretching of arterial walls, but the pathogenesis of ischemia is unknown. It is important to know that in some situations, manipulation of the neck may do more harm than good. Your Physiotherapists will carefully check your neck before manipulating it to see if other methods, such as mobilisation would be preferable.
Sporting technique and rehabilitation
Correct technique especially in swimming, racquet sports or throwing sports has significant contribution in preventing "overuse" type of cervical injuries from occurring. For example, a tennis player who has poor thoracic and lumbar mobility and abnormal scapulothoracic and glenohumeral mechanics will stress her/his cervical spine more often during serving and overhead shots as she/he tries to maximize her/his reach and power. This can result in cervical overuse syndrome. The Sport Physiotherapist should assess and discuss any faulty techniques with the coach and prescribe appropriate rehabilitation programme.
The content of this leaflet is provided by:
Sports Medicine Department, Athlete & Scientific Services Division, Hong Kong Sports Institute
For more information, please contact:
Sports Medicine Department
Telephone: (852) 2681 6134
All information in this pamphlet is for reference only