 ID: hksportsinstitute
ID: hksportsinstitute

Sports Medicine Education No. V - Plantar Fasciitis
Description
Plantar fasciitis is a common injury in sports which involve running or jumping. It is an inflammation of the plantar fascia which is usually caused by microtears in the plantar fascia near its attachment to the heel from repetitive trauma. The longer the inflammation lasts, the greater the possibility a bone spur will develop. However, there are also people who have got bone spur but no heel pain.
Sufferers complain of pinpoint, knife-like pain in the heel sometimes with a deep aching or burning pain spreading distally along the medial arch. The pain is usually worse in the morning or after prolonged sitting. In the early stage, pain improves with warm up and use but it will often progress into a situation where there is pain on activities of daily living. Runners may alter how they run in order to avoid pain: shortening stride length, foot striking with toes first rather than heel first, and running on the outside border of the foot etc. These alterations may lead to other problems such as knee pain, hip, back pain and/or other foot pain.
Anatomy
Plantar fascia is the thick fibrous tissue that runs from the heel to the bases of the toes. It supports the joints, bones and muscles under the foot during midstep and creates a rigid lever for push-off. It maintains the longitudinal arch of the foot.
Rish factor
Studies found that a lot of the runners' injuries were associated with training errors and excess mileage. These training errors include:
- increase in mileage over a short time
- intensive workouts (e.g. interval training on a hard surface wearing spiked shoes)
- sudden increase in hill running
- increased frequency of workouts
- running on surfaces with either too much or too little resilience (concrete, asphalt, grass, sand etc)
- running on banked or crowned surfaces
- inadequate recovery time
Other factors which predispose runners to plantar fasciitis include:
- lack of strength and flexibility in the ankle and foot
- high arches or flat feet
- bowlegs, knock knees, tibial torsion, leg length differences, rotation of the hip sockets
- deficiencies in running shoes (too flexible, toe boxes too tight, soles to rigid, inadequate arch support and shock absorption etc)
Treatment and management
- Active rest: decrease mileage by 25-75%, minimize sprinting and avoid hill running. If pain is severe, running might need to be stopped completely. Swim, run in water or ride a bike instead.
- Physiotherapy: ice and electrical modalities to reduce pain and inflammation; manual therapy to improve foot mechanics.
- Stretching exercises. (hamstrings, calves, plantar fascia)
- Strengthening exercises. (calves, intrinsic muscles of feet)
- Orthotics: heel lifts, heelcups or arch supports to improve suport and shock absorption.
- Taping: temporarily support the arch and decrease the stress on the plantar fascia.
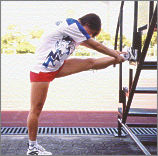
hamstrings stretching exercise
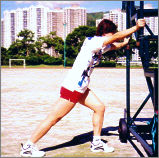
calf stretching exercise

calf stretching exercise
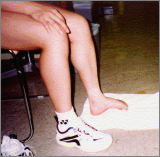
towel gripping exercise to strengthen intrinsic muscles of feet
Low Dye taping
Return to sports and prevention of recurrence
When pain and tenderness decreases, you can resume training but with less mileage, lower intensity and on softer surface. A useful guideline for a safe progression is the "10%" rule, i.e. limit increase in distance or intensity to 10% a week. For example, if a person is running 60 minutes a session, 4 times a week (i.e. 240 minutes in total), he or she can probably increase the running time to 264 minutes (240 + 10%) the following week if all else remains the same.
Remember even good shoes will lose their shock-absorbing qualities after frequent use, e.g. 40% is lost after 250 to 500 miles! Old worn out shoes should be replaced.
Follow your exercise regime prescribed by the physiotherapist and seek for further advice if pain persists or recurs.
For more information, please contact:
Sports Medicine Department
Telephone: (852) 2681 6134
All information in this pamphlet is for reference only